#Parathyroid hormone
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. has $15.1M in annual revenue.
Text

The Science Research Notebooks of Satyendra Sunkavally, p 543.
".......od paet him aeghwylc para ymb sittendra...."
_Beowulf
#essential fatty acids#cortisol#fibroblasts#salt water#conduction of sound#unsaturated fatty acids in the diet#hormone receptors#parathyroid hormone#monoamine oxidase inhibitor#alcohol#coffee#amines#Beowulf#manuscripts
0 notes
Text
About blasts, clasts and receptors: PT H in the bone cannot be erased, yet GPRC5 is not tALK-3 with other signals
Osteoporosis is a skeletal condition that leads to the weakening of bones, making them porous, fragile, and prone to breakage. A whopping 8.9 million fractures are caused by osteoporosis annually. The aging population is the most vulnerable to primary osteoporosis, given, their frailty, and often, requires long-term therapy and support. Advances in healthcare and the corresponding rise in the…

View On WordPress
#bone density#bone fracture#bone strenght#cell receptor#cellular signaling#osteoblasts#osteoclasts#osteoporosis#parathyroid hormone#teriparatide
0 notes
Text
The U.S. and European Union Osteoporosis Drugs Market Is Driven by Increasing Prevalence of Osteoporosis
The U.S. and European Union osteoporosis drugs market is experiencing growth, and this development can be credited to the growing occurrence rate of osteoporosis illnesses, the rising elderly populace, the rising cases of overweightness, the increasing occurrence of lifestyle-related illnesses, and the rising healthcare expenditure in the U.S. and the EU. In 2022, the U.S. osteoporosis drugs…

View On WordPress
#Bisphosphonates#European Union Osteoporosis Drugs Market#Parathyroid Hormone Therapy#RANK Ligand Inhibitors#SERMs#U.S. Osteoporosis Drugs Market
0 notes
Text
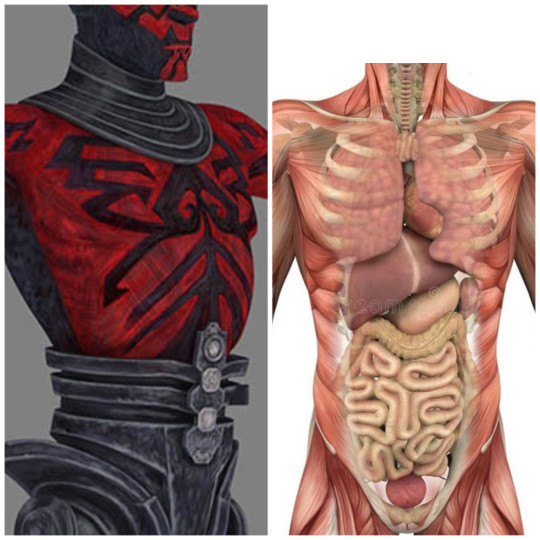
For fun, I wanted to think through which organs Darth Maul is actually missing. This gives us clues as to which bodily processes he just doesn't have anymore, which ones he's using sith juju to make up for, and what Talzin or Death Watch might've done for him with the prosthetics. To be fair, humans have about 70 to 80 possible organs systems (don't ask), but who knows what zabrak have, and where they truly are located. We can only guess.
✓ Means he probably has this.
X Means he probably doesn't have this.
O Means he probably only has some.
(Checklist and conclusions below the cut.)
✓ Adrenal glands (above the kidneys)
X Anus
X Appendix
X Bladder
O Bones
O Bone marrow (spongy part of the bone)
✓ Brain
✓ Bronchi (tubes in the lungs)
✓ Diaphragm (muscle of breathing)
✓ Ears
✓ Esophagus
✓ Eyes
✓ Gallbladder
X Genitals
✓ Heart ( 2 of them!)
✓ Hypothalamus (in the brain)
O Joints
✓ Kidneys
O Large intestine
✓ Larynx (voice box)
✓ Liver
✓ Lungs
O Lymph nodes
O Mesentery (Nerves, vessel, & fat storage in gut)
✓ Mouth
✓ Nasal cavity
✓ Nose
✓ Pancreas (hormones/enzymes)
✓ Pineal gland (in the brain- hormone production)
✓ Parathyroid glands (hormones, in the neck)
✓ Pharynx (back of the throat)
✓ Pituitary gland (in the brain, hormones)
X Prostate
X Rectum
✓ Salivary glands
O Skeletal muscles
O Skin
O Small intestine
O Spinal cord
✓ Spleen (big blood filter)
✓ Stomach
✓ Teeth
✓ Thymus gland (immune training, in the chest)
✓ Thyroid (hormones, in the neck)
✓ Trachea
✓ Tongue
O Ureters (Kidney to bladder tubes)
X Urethra
O Ligaments (connect muscles to bones)
O Tendons (connect bones to bones)
✓ Blood cells
✓ Hair (Uhhh... horns? I guess he has eyelashes?)
✓ The vestibular system (of the ear)
X Testes (unless zabrak locate them internally)
✓ Nails
X Vas deferens (testes to genitals tube)
X Seminal vesicles (semen fluid production)
X Bulbourethral glands (makes preejaculate)
X Penis
X Scrotum (if zabrak keep the testes externally)
✓ Parathyroid glands (neck, hormonal)
O Thoracic ducts (Where lymph flows into veins)
O Arteries
O Veins
O Capillaries
O Lymphatic vessels
✓ Tonsils
O Nerves
O Subcutaneous tissue
O Olfactory epithelium (nose)
✓ Cerebellum
Long story short, besides just his legs and genitals, Maul lost most of his digestive and urinary systems.
He actually kept almost all of his life-critical organs, so whatever sith voodoo he was doing to stay alive on Lotho Minor was probably focused on fighting off sepsis (due to the unclean end points of his digestive system. Remember he got cauterized by a lightsaber so assume he had to make... new holes. There may have also been some self-done surgery to reconnect what remained of his large and small intestines.)
The loss of his testes, if he indeed had human typical location for them, could have proven a growing problem, considering that they make 90% of a man's testosterone, and that's needed just to have normal amounts of energy.
The digestive track is also a problem, as the gut microbiome is where a lot of neurochemicals are produced. For example, 95%~ of the body's seratonin is produced in the gut. Lacking huge chunks of his small and large intestine means that Maul had poor absorbtion of nutrients, and probably needed to eat all the time just to get a fraction of the calories and nutrients from his food.
So. He lived on the edge of starvation due to a truncated digestive track, had low energy, mood imbalances like you wouldn't believe, and constant sepsis. I'm sure the acid rain being the only source of fresh water was also just, so helpful.
I assume, by the lack of black veins on him afterward, and (sort of?) stable mood, that talzin might've regrown some of his gut and fixed the end point issues. Later on, Death Watch (being mandalorians) might've given him more robust life support systems that included testosterone replacement and cybernetic genitals. Seems like what they would do for their own people.
Possible lingering complications? I assume he has a VERY weird relationship with food. He had spider legs for twelve years, so bipedal motion probably fails him sometimes. Back pain. Phantom leg pain. Nerve junction issues. Immune system weirdness (from all that missing marrow, and a long stint with sepsis). Issues storing fat. Talzin yoloed his brain back to sane-adjacent, so mental health is... I mean. Yeah. Triggers. Teeth prone to chipping and cavities (from malnutrition and acid water). Possibly goes to the bathroom once a day and urinates like a race horse. Issues with being touched, myriad phobias, and a squirrelly libido.
Did I miss anything?
#darth maul#star wars#maul opress#nightbrothers#zabrak#sith#lotho minor#writing resources#fanon#medical#xenobiology#sci-fi healthcare
261 notes
·
View notes
Text
Yandere!Thrawn x F!reader chapter 9

Yandere AU - 2 - 3 - 4 - 5 - 6 - 7 - 8
Tags : Yandere behaviors (duh), starday, negociation of bondaries
Thrawn opens his very special package and smiles to himself. It is quite hard to get those hormones, because they’re prohibited first off and after because they are an ingredient of the latest trendy hallucinogenic drugs on Coruscant. People kill for them.
For him they have the very neat effect of slowing down considerably the parathyroid hormone production, preventing a swiftly recovery of fractures and fissured bones. You don’t know it but he laced all your dishes with it, slowing down your recovery. You should take more than 10 weeks to recover instead of the standard 6 to 8 weeks. All of that is bonus time with you for him!
But he’s curious about the hallucinogenic effects too. He may try them on you as a reward or punishment, he doesn’t know yet. He dusts the powder on the icing of the cake.
Today is your starday! He would never forget such a date, he planned a nice dinner, a present and a romantic movie to watch together after. Or he will let you think you choose a romantic movie yourself, but he thought about it for several weeks ahead.
“(Y/n), it will be time to bathe you.” he announces to you with a stoic voice as he enters the bedroom, hiding his excitement. “Oh… Okay…” each evening you have the crazy hope you will escape it, each evening he undresses and massages your body meticulously to clean it. He knows you don’t like it, but you surrendered by now, you know, deep down, that you can’t escape him and so you stopped making it complicated for him. You’re not relaxed under his hands yet but it is easier now.
You curse that time of day while he can’t wait for it. Each evening he takes pleasure in choosing in which soap he will bathe you today, adding oils and perfume and special body cream to make your skin smooth (all under the pretenses it will ease the pain of your bruises of course.)
You’re suspicious of him of course. Who wouldn’t in your situation? That is why he takes care to not spend too much time on the erogenous zones of your body, despite his deepest wishes, and to clean your whole body thoroughly. He chooses modest garments to dress you, with just one slit here and there, nothing too suspicious. He washes your underwear that he steals from you regularly so you don’t notice them disappearing. He never touches you more than necessary, he might have just taken a handful of your plump thighs in his hands, but come one, he just needed to find a good grip on you to carry you!
One day you flatley refused to be bathed, plain and simple. You turned your back to him, crossing your arms. He was, of course, prepared for that eventuality. “May I know why?” He asked calmly but with authority, “Because this is terribly humiliating!” You exploded “You see me naked each and every day, I feel exposed and violated! And the way you touch me…”, “I do not remember touching you in an unreasonable way.” he says like he doesn’t see the problem and you are being the unreasonable one. You just shudder, “Yeah,I know. But still, this crosses my boundaries in so many ways! I would rather we stop.”
Like hell he will stop.
“I do not see the problem.” He flatly responds. “In the Ascendancy we bathe all together to strengthen the bonds between family members and friends in hot springs.” he recalls, a hand on his chin. That must be his most outrageous lie to date, “We are more modest here.” you counter “We do not show our naked body to simple friends.”, “I see.” he continues, “But I have a different view of modesty and nakedness than humans, we are not shy about it, we see it as a simple aspect of life and of a body. Nothing to be shy or embarrassed about. I have bathed naked with numerous female colleagues and friends before.” You slowly turn your head towards him with pursed lips, he tilts his head to you. “This is a very asexual activity for all of us, free of judgment and ambiguity.” It couldn’t be more false, Chiss are as conservative if not more than humans on that subject.
You look into his eyes to see if he is lying, as usual his gaze is clear and resolute and you can’t get any info out of it. You bite your lips, “Even if you say that, it doesn’t help the shame I feel.”, “The shame of what? Being vulnerable with a friend?”, “To be powerless! I’m an officer of the Empire and can’t do anything on my own right now!” you shout, annoyed. “(Y/n), this is a simple bad patch. You will heal and recover your power. You just need the assistance of a friend.”, “Well it is humiliating!”
“Would you have preferred a human colleague to do it instead of me?” He taunts, pretending to be compassionate. You remain silent, thinking. “No. In retrospect it is better if it’s you.” You admit “You wouldn’t… You would never take advantage of a situation. I trust you.”
And this, this is why you let him do it. Because he succeeded to convince you that he is better than this, that he is upright and a man of honesty that would never hand on a woman in any way shape or form. He is the ever the stoic Grand Admiral Thrawn after all, he is known to be brutally honest and direct. And that is true, to a certain extent. He would never take advantage of a situation over anybody, even his former partners. If one man would never be bothered and interested by such basic needs and desires, it’s him.
But they weren’t you. They didn’t have your perfection. They weren’t his darling… They didn’t obsess his mind like you do, plaguing him at all hours of the day and night.
You can’t see him behind you but he’s grinning at your words. How you blindly trust him, believing in his personna so fully, after all he mastered the mask for years. Not even Eli has the slightest idea of what is going on in his mind. All the emotions raging on behind the meticulously crafted aloof and disinterested expression, all the perverted fantasies that kept brewing within him since his younger age. How would you be able to see right through him?
He has some “mishaps” here and there but you make quick excuses for them because he is just above any suspicion. You never saw him hitting on someone, caressing someone, seeing any true inner desires appear through, he must be above baseless desires and romantic sentiments! He forces you to appear naked before him? His relationship to modesty and nakedness are fundamentally culturally different, what are you gonna do? Fly to the Ascendancy to check? He massages your naked body with body cream each evening? It is obviously to soothe your bruised skin, there is nothing weird here, why do YOU feel the need to make it weird? He helps you eat like a mother helps her young child, infantilising you? You’re in a cast, how do you expect to eat with dignity without your dominant hand? He joins you in bed each night, pressing your two bodies together like a couple would? You’re the one complaining it was cold in the first place, why are you always dissatisfied with the solutions he proposes?
He’s just trying to help you, why do you always feel the need to make it difficult for him? Him who takes time off his crowded Grand Admiral agenda just to help you. Aren’t you a spoiled and ungrateful woman to question his actions?
Every time you have a concern or a reluctance he looks at YOU like you're the crazy one, why looking into it? He raises an eyebrow, looking at you like an animal in a cage going in a frenzy, why are you always questioning his good intentions? Him who saved your life! How ungrateful can you be! He’s simply trying his best to help his friend, why give him bad intentions? Why look into his actions suspiciously? Him who forgave you your treachery. Isn’t he a saint to both forgive you AND helps you out of your misery? He’s not obligated to do that after all, if he’s fed up with your antics he could very well send you back to the med bay, at the mercy of your tormentors without any protection. How can you even doubt him? If we look at it he is the true victim between you two.
This is what you’re torturing yourself with each sleepless night, feeling his warm body pressed against your back. Rummining each and every little action like you’re the crazy one. All those gut wrenching doubts clashing with the proper and honest portrayal you have of him.
But that is what he wants you to do. To doubt your own feelings and very well justified fears. To lose grips on what is truly acceptable and what is obviously crossing a justified boundary.
So you let him do it… You stopped fighting and lowered your defenses. You just grit your teeth and suck it up while he takes his twisted pleasure in forcing you to submit. Tonight will be no exception. He lifts you off the bed and heads toward the bathroom.
Once this is done he dresses you in a fancy dress with sparkle and lace and not your usual pajamas. You tilt your head to him, eyes full of questions. “You did not think I forgot what day it is?” He asks you with a lopsided grin, “I planned a delicious soiree for us both.”
He carries you to the living room where a gentle music plays, dim lights create an intimate atmosphere, a candelabra burning on the table overflowing with food. “Happy Starday, my friend.” He says softly, laying you on your attributed chair, “I took the liberty to ask for dishes from your homeworld, to make you feel at home, at least a little bit.”, “Oh Thrawn…” You murmur emotionally “This is… You shouldn't have! It is too much!”, “Come on now, there is no “too much” when we celebrate a friend.” He counters, opening a bottle of champagne, “I know you the crew celebrate each starday with a little party, I wanted to know how it feels like.” He simply explains. You feel an icy feeling at the bottom of your stomach, those little parties are reserved for the crew members and some ensigns, typically the hierarchy doesn’t get involved so Thrawn was never invited.
Did he… Did he wanted to come? To celebrate with all of you?
“Thrawn I-” you start but he cuts you with a gesture of the hand, “I know you don’t want your superiors to mingle in those parties. I understand it. I just thought today would be a good occasion to enjoy it at a lesser level.”, “Thrawn, I am sorry.” You offer, sympathetic, “If we knew… If I knew you wanted to enjoy those parties I would have invited you. But I didn’t think you would even care, you’re always so detached from everything.” You bite your inner cheek, how many evenings did he spend in complete solitude while you partied, getting drunk on cheap booze with friends?
“No need for excuses, Cha’cah. You are here tonight, that is what matter.”, “No, Thrawn really! We would have welcomed you if you’d asked!” You feel like such a bad friend now… You never once checked on him to know if he wanted to party. “Let us focus on you tonight.” He cuts the conversation short, “I hope it will taste good, I cooked some of the dishes.”, “You…? Oh maker, and I’m not even sure what the date of your starday is…” You hide your face in your hand, absolutely mortified. Wow, you are such a miserable friend! It’s a real mystery what he even sees in you.
You just hear a light chuckle in response. “You have all the time in the world to memorize it.” He serves you both and starts cutting your roast to manageable pieces. He picks one piece with the fork and extends his hand to you, “No!” You say firmly, “Let me try.” You seize the forks with your non-dominant hand and bite into it, your movements are unsure and clumsy but you manage to eat your meat on your own, absolutely determined to not let yourself get pampered and getting some autonomy back! You smile at your success “Hell yeah, look at that! It’s less easy than you can believe!”
He observes you with a false smile. Why are you trying to eat on your own? Why not let him do it? You had such a thing going on, why try to rob him from it? He will ask for more difficult dishes to eat from now on. He eats little bite by little bite, observing you finishing your plate with your stupidly blissful smile on your face. Why are you so happy about getting away from him, even for an inch? Everything was so perfect and now you can’t think of anything else but leaving him behind!
But he smiles, a gentle smile, a smile friends give when another progresses. But his eyes don't sparkle. He’s ruminating while you speak enthusiastically, at least this little dinner is giving you back some life… He, at least, gets to enjoy your laugh.
He opens the cloche for the desert and your eyes open wide. This cake… It is the cake you asked your mother for each year when you were young. A favorite of yours you didn’t have in years.
“How did you knew?” You ask incredulously, “I did my little investigation.” He answers enigmatically.
He is in contact with your family for months now. He knows where they all live and have their personnel numbers. He talked to them for weeks, presenting himself as a friend of yours. Well, that isn’t lying, no? He even talked to your homeworld friends, he decorticated your life from every angle, examining you under a microscope behind your back.
“Oh maker, that scent… So many memories.” You utter, lost in your memory. He lights up the candles and pushes the cake towards you, you can’ help but chuckle, “Thrawn, I’m not a kid anymore.”, “Humor me, I find this tradition with candles most interesting.” You blow the candles out and claps, thoroughly amused, drooling at the simple sight of your favorite childhood cake. You try to cut two parts yourself, just managing to mash them, destroying the presentation completely, “Oh no!” you laugh. You eat, your hand trembling, but with a smile on your face.
Once you’re finished and avidly licked your plate of all the cream he takes out a velvet box that he hands you with a gentle smile, “Happy Starday, my friend.”. He opens it with a “click” letting you admire a golden choker with little white diamonds sprinkled on it, something is engraved and a little chain dangling, making a hoop, at the center, harmonizing the piece. You touch it with the tip of your fingers, eyes wide open and sparkling.
“Oh wow…” you can only say. “Do you like it?” he asks, “It’s beautiful… What is engraved?”, “It is your name in cheuhn.” he explains, rising of his seat to put in on you.
It is not your name. It’s written “my cha’cah” in cheuhn. You don’t need to know, but he will see his claim on you each time you decide to wear it, proudly announcing to the world that you belong to him. And he can't wait to attach a chain on the little hoop…
“May I ask the price?” You ask, worried. “No you cannot. It is improper to reveal it.” He shuts you down with a smile in his voice. He paid it a little fortune, but you’re so worth it! He chose the most expensive precious metals and diamonds just for you…
He carries you to a mirror for you to admire yourself. “So this is how my name would be spelled in Cheuhn?” You ask curiously, “Yes.” He lies with a thin smile, “You wear it perfectly.”. You admire yourself a little more and ask him to take it off, “Why?” he asks confused, “I just don’t want to scratch or damage it.” you explain, raising your valid hand to try and unclip it. “Please.” he seizes your hand mid movement delicately “Wear it a little more, I want to admire it on you.” You look at him surprised, but oblige, it isn’t unreasonable. So you keep it, letting him admire you with what’s basically a dog collar with his claim on you. He can’t keep his eyes out of your precious adorned neck, devouring you with his gaze like a salivating predator.
Oh you are so beautiful like that…
It only misses the chain with what he could tugs you closer to him, choking you a bit, hearing your delicious gasp as you are being pulled in his embrace. He can’t wait to make love to you with it shining on your neck.
You mind absently touch it from time to time, it is just a little too tight making it a little difficult to breathe in. Just as he asked the jeweler.
To finish the soiree he carries you back to the bed where he puts on a romantic movie. He doesn’t like them especially, too sappy for his taste, but he knows you’re an avid watcher of the genre. So he will gladly oblige, for you he will go to the other side of the universe, so watching some mushy movies is a piece of cake. He very gently, very slowly, passes his arm around your shoulders, pressing you close to him as you sigh away at the main lead declaration to their lover. “Isn’t it beautiful?” you ask “To devote yourself to someone to such an extent?” your eyes are glued to the screen, not noticing that his red burning rubies are on you and not the TV. “I guess it is…” He sighs, lost in your beauty, so close and so far away.
But not for long now…
He just needs to be a little bit more patient and you’ll be his forever.

@bluechiss @blueninjablade3 @al-astakbar @thrawnspetgoose @readinglistfics @twilekchiss @pencil-urchin @ineedazeezee @mssbridgerton @dance-like-russia-isnt-watching @Cortisolcosplay
☆Tag list
#yandere au#thrawn x you#thrawn x reader#thrawn x f!reader#thrawn#grand admiral thrawn#mitth’raw’nuruodo#fanfic#vibratingskull
46 notes
·
View notes
Text
Since we're back on the topic of health, has any of you ladies dealt with low phosphorus in blood?
I asked my doctor to test me for calcium, because I'm always freaking out about calcium, and she also checked me for phosphorus, and it turned out calcium is just a tiny bit low, but phosphorus is low, and now I'm being tested for parathyroid hormone, which as far as I can tell, controls how the calcium is regulated in the body.
I've been reading on what low phosphorus means and it's like, horror stories, freaked me out, so I've decided to ignore all that, and act like things are fine :) the very best thing to do for health anxiety :) it can't be that bad :)
#health issues#i love how nobody explains anything to me in health industry#they just throw big words at me as if i understand any of that#later i get to look them all up#and still not understand
11 notes
·
View notes
Text
Propaganda!

The cytoskeleton is a complex, dynamic network of interlinking protein filaments present in the cytoplasm of all cells, including those of bacteria and archaea. In eukaryotes, it extends from the cell nucleus to the cell membrane and is composed of similar proteins in the various organisms. It is composed of three main components: microfilaments, intermediate filaments, and microtubules, and these are all capable of rapid growth or disassembly depending on the cell's requirements.
The Indian hedgehog protein is one of three proteins in the mammalian hedgehog family, the others being desert hedgehog (DHH) and sonic hedgehog (SHH). It is involved in chondrocyte differentiation, proliferation and maturation especially during endochondral ossification. It regulates its effects by feedback control of parathyroid hormone-related peptide (PTHrP).
#Cytoskeletons#Indian hedgehog (Ihh) protein#tournament poll#polls#wikipedia#cells of the human body#science tournament#biochemistry
4 notes
·
View notes
Text
Sickle cell nephropathy, a complication not to be ignored, through a Moroccan case by Asmaa Biaz in Journal of Clinical Case Reports Medical Images and Health Sciences
Summary
Nephropathy is a major complication of sickle cell disease. Indeed, the kidneys are particularly sensitive organs to this disease.
We report a case of a patient with a major sickle cell syndrome; she was hospitalized in the nephrology department of Mohammed V Military Training Hospital, forend-stage renal failure. The family investigation revealed a composite S/O-Arab heterozygosity responsible for the severity of the clinical disorder.
Key words: Sickle cell nephropathy - End stage renal failure - Sickle cell major syndrome S/O-Arab.
Introduction
Sickle cell nephropathy (SCN) is a major complication of sickle cell disease. It manifest’s in various forms, including glomerulopathy, proteinuria, hematuria, and Renal tubular disorders, and frequently results in end-stage renal disease(ESRD). Hemolysis and vascular occlusion are the main factors promoting the manifestations of this disease. Dialysis and renal transplantation are the last resort for patient with SCN [1].
Through the case of a patient with a major sickle cell syndrome S/O-Arab complicated by end-stage renal failure, we will explain the pathophysiological mechanisms of this complication and emphasize the importance of biological monitoring.
Case report
The patient was 24 years old and was admitted to the nephrology department of the Mohammed V Military Training Hospital for incidental renal failure in the context of an impure nephrotic syndrome revealing sickle cell nephropathy. In his history, we retained a
follow-up since the age of 5 years in another hospital structure for a hemoglobinosis S treated by iterative transfusions with notion of acute renal failure during sickle cell crises.
The biological result showed an anemia at 7.7 g/dL, corrected serum calcium at 82 mg/L, serum phosphorus at 64 mg/L, intact parathyroid hormone 1-84 at 543 pg/L, Alkaline Phosphatase at 201 U/L.
Hemoglobin electrophoresis was ordered to this patient, but due to repeated transfusions, her electrophoretic profile remains uninterpretable. Therefore, hemoglobin electrophoresis (HBE) was performed in the parents as part of the hemoglobin phenotypic study. The HBE of both parents is performed on Capillarys (Sebia®) at alkaline pH followed by electrophoresis at acidic pH on Hydrasys (Sebia®) which showed a heterozygous Hb O-Arab variant in the mother and a heterozygous hemoglobinosis S (A/S) in the father.
Referring to the phenotypic study of Hb performed in the parents, it is concluded that the patient has a composite heterozygosity S/O-Arab explaining the severity of the renal manifestations.
The evolution was marked by the absence of improvement of her renal function and the aggravation of the uremic syndrome motivating her setting in peritoneal dialysis. The patient was treated with erythropoietin ARANESP 30µg/ per 2 weeks with a blood transfusion of 2 packed red blood cells on average every two months.
The patient died at the age of 26 years before benefiting from either a hemoglobin genotyping study or a renal transplant.
Discussion
Sickle cell disease is the most common hereditary hemoglobinopathy in the world. An estimated 300,000 children are born with this disease each year, three quarters of whom are born in sub-Saharan Africa [2]. It is characterized by extreme variability in terms of clinical manifestations, the most serious of which are renal manifestations.
The association S/O Arab is responsible for a major sickle cell syndrome, as in the case of our patient. Indeed, Hb O Arab stabilizes the intracellular polymerization of Hb S and leads to an irreversible sickle cell disease of red blood cells, thus expressing by a more severe clinical disorder. The clinical and biological manifestation of this association is similar to homozygous sickle cell disease and the association Hb S / Hb D Punjab. The onset is usually early, in infancy, and is marked by the classic triad of chronic hemolysis: anemia, jaundice and splenomegaly. Anemia is usually moderate outside of hemolytic attacks (Hb = 7 - 10 g/dL). The evolution is often marked by sickle cell complications. Osteoarticular complications are the most frequent, such as vaso-occlusive crises, septic arthritis and osteoporosis. Pneumonia, leg ulcers and vesicular lithiasis are also reported [3].
Sickle cell nephropathy is a major complication of sickle cell disease. The kidneys are particularly sensitive organs to the disease. Sickle cell disease substantially alters the structure and function of the kidneys and is the cause of several renal diseases and syndromes. Renal damage is more severe in SS homozygous patients than in other major sickle cell syndromes [4]. Approximately 5-18% of patients have SCN, thus increasing the risk of morbidity and mortality of the disease [5].
A number of studies have focused on this pathology, its evolution includes several stages; it starts with hyperfiltration, then the occurrence of microalbuminuria, then macroalbuminuria and finally the progression to renal failure. The prevalence of these complications increases with the age of the patients but can also be seen from a young age.
Two models have been proposed to explain the pathophysiology of SCN. Becker et al. showed that prostaglandin release following ischemic injury causes an increase in glomerular filtration rate (GFR). This increase leads to glomerular injury and eventually manifests as proteinuria and glomerulosclerosis [6]. Alternatively, Nath and Katusic [7] classified the manifestations of SCN into two different phenotypes: the hemolysis-endothelial dysfunction phenotype and the viscosity-vaso-occlusive phenotype. The hemolysis-endothelial dysfunction phenotype affects the renal cortex and leads to hyperfiltration and glomerulopathy; heme released due to intravascular hemolysis predisposes to proteinuria through its accumulation on the glomerular filtration barrier, which disrupts membrane selectivity by exerting cytotoxic effects on podocytes and endothelial cells [8]. On the other hand, the viscosity-vaso-occlusive phenotype is responsible for hematuria, papillary necrosis, and tubular acidosis [9].
Microalbuminuria, reflecting the early stages of renal damage, should be routinely sought in the follow-up assessment in this category of patients.
Decreased GFR, which suggests loss of kidney function, occurs with the progression of sickle cell disease and may be a sign of uncontrolled disease. Sickle cell patients have a higher risk of developing chronic kidney disease compared to the general population.
Specific treatment with an angiotensin-converting enzyme inhibitor or an angiotensin II
receptor antagonist should be considered in these patients in order to slow the progression of the renal disease. The prevention of microthrombosis and thus of renal damage requires the maintenance of a hemoglobin A level of more than 50% by regular blood transfusion as soon as sickle cell disease is diagnosed. The role of hydroxyurea in the prevention and/or treatment of renal function abnormalities in sickle cell disease remains to be studied [10].
Conclusion
Sickle cell nephropathy is a major complication of sickle cell disease. It must be systematically and early sought in all sickle cell patients to reduce the risk of morbidity and mortality of this disease.
The development of new biomarkers has become increasingly essential for the early detection of sickle cell disease in order to improve the survival of patients with sickle cell disease.
Declaration of interest:
The authors declare no conflict of interest.
#Sickle cell nephropathy - End stage renal failure - Sickle cell major syndrome S/O-Arab#JCRMHS#Is Journal of Clinical Case Reports Medical Images and Health Sciences PubMed indexed.#clinical decision making#clinical images submissions
3 notes
·
View notes
Text

TSRNOSS, p 468.
#Addison's disease#lithium#neutrophils#inborn errors of metabolism#magnesium#parathyroid hormone#hypocalcemia#calcification of the basal ganglia#calcification of the amygdala#lithium ion#neutrophil production#calcitonin#osteoporosis#lathyrism#collagen crosslinking#satyendra sunkavally#theoretical biology#manuscript#cursive handwriting#British flowers#nectar#metabolic rate
0 notes
Text
biologically accurate deergirl who transitions and ends up developing masses and tumors all over her body along with unchecked antler growth and the inability to shed due a drop in testosterone causing a parathyroid hormone imbalance which halts calcium absorption. but on the bright side her muscle mass has atrophied significantly and she is less aggressive around breeding season
2 notes
·
View notes
Text
psych unit 3 (biological psychology) review!!! part A, 2/2
THE NERVOUS SYSTEM is broken up into several subdivisions:

the nervous system in general is the body's (main) communication system. the central nervous system is just the brain and spinal cord, which communicates with the rest of the body via the peripheral nervous system. the spinal cord part of the CNS is responsible for reflexes; the information, ex. pain signals, reaches the spinal cord before the brain, which then responds immediately, meaning your body can respond before your brain even processes the initial information! neat! the "manual" part of the peripheral nervous system is called the somatic nervous system, which is used for voluntary movement, while the "automatic" part of it is called the autonomic (crazy i know) nervous system, which controls involuntary movement like internal organ and gland activities. the autonomic nervous system is also divided into two, the sympathetic and parasympathetic nervous systems, which are responsible for arousing (stress response arousal not freaky arousal!!!) and relaxing the body respectively.
THE ENDOCRINE SYSTEM is the other communication system. while the nervous system uses quick signals, the endocrine system uses hormones, which are comparatively much slower, since they travel through the bloodstream, but longer lasting.
the nervous and endocrine systems are super interconnected!! for example, the autonomic nervous system can tell the adrenal glands (the ones on your kidneys) to release adrenaline/epinephrine and noradrenaline/norepinephrine during a stress response. the most important gland, though, is the pituitary gland in the brain, controlled by the hypothalamus (more on him later...). it influences growth and other glands with its hormones.
other parts of the endocrine system include the thyroid glands, which influence metabolism; the parathyroids, which regulates blood calcium levels; the pancreas, which regulates blood sugar levels; and the testis and ovaries, which secrete male or female sex hormones. this is a psych class so idk anything deeper about any of that but! maybe when we get to it in bio.
part A done yay! part B is about actual brain structures and imaging techniques!!! my favourite
4 notes
·
View notes
Note
I have decalcification I'm gonna cry. Why am I telling you? Because it 4:39 am on a school night and I need someone to annoy other than my hom
I don't know why you are telling me about this, I am not the doctor of this duo. But he is most likely asleep already, so fine, I'll humour you. Are you talking about your bones, your teeth, or both? Sounds like you might have a vitamin D deficiency, that can lead to decreased bone density and hypocalcemia. You should get your vitamin D blood levels checked, but also your parathyroid hormone (PTH) as this also is involved in bone density and calcium homeostasis. Vitamin D gets produced in the skin when it's exposed to sunlight, so spending more time in the sun could also help, but you will most likely get vitamin D supplements if you are deficient, this helps absorption of calcium in the intestinal tract and retention in the kidneys.
#this is not medical advice dont take me serious im just like wikipedia or chatgpt throwing information at you because i am bored#rp#roleplay#sherlock rp#sherlock roleplay#sherlock gives advice#might be bad or not but you all ask for it#john also forces me to take all this suplements because i am deficient
10 notes
·
View notes
Note
*turns a page in my notebook and changes pen colour*
What is your logic for why ghoul coagulation works on phosphorous versus calcium for humans?
I’m so glad you asked! It’s a whole can of worms that involves me getting wild about clinical chemistry so buckle in. ♡
Part of it stems from I love the idea that after summoning ghouls there was this period of rediscovery and adjustment in thinking physiology wise. I wanted there to be a reason to develop new ways of doing stuff specific for ghoul health. They are rather humanoid creatures that have been put into human vessels, but i love the idea that their physiological processes work just ever so slightly different from what was expected. Most anticoagulants that are used in blood collection tubes work by inhibiting calcium in some way (cause it activates both platelets for clotting but also large parts of the coagulation pathway) so replacing calcium in coagulation is a small change that shakes everything up so much! Ghouls not utilizing calcium in coag is honestly an excuse for me to have fun with biology.
I do have both lore and actual science reasons for picking phosphorus in particular. In serum chemistry (chemistry related to the non-cellular part of blood, so like the plasma and all the various minerals/proteins/hormones etc floating around inside it) calcium and phosphorus act in an inverse relationship. So as calcium levels go up, phosphorus goes down. They are intrinsically linked together and balance out in combination with action of Magnesium, Vitamin D, and parathyroid hormone (but that’s not the point). Therefore I was like oh if ghoul blood isn’t utilizing calcium in clotting, then it should be it’s buddy phosphorous so everything is almost the same, but opposite at the same time, and went off fantasizing and theorizing from there.
Normally calcium levels are slightly higher than phosphorus in humans, but in ghouls it would be reverse. There would be a survival advantage of this too. Sources of phosphorus would be a lot more common in hell, but ALSO calcium needs Vitamin D to absorb correctly. By working on a phosphorus based clotting system instead of calcium, it would then require less calcium in the body and therefore less direct sunlight for activation of vitamin D to absorb that calcium.
After I thought all that out I also realized that by decreasing the need for calcium and making phosphorus more prominent there would also be bone chemistry effects. Cause the reason you hear “oh drink milk for healthy bones” is because your bones act as a calcium storage spot and if depleted too much makes for weaker bones. In theory if there’s decreased calcium need and increased phosphorus circulation, it could be argued that ghouls have stronger bones than humans (cool!).
#ghoul blood stuff#nocturnal lore corner#nocturnal asks#askingforthesun#ghost headcannons#the band ghost
7 notes
·
View notes
Text
Trusted Oncological Care With Trusted Hands

It is but natural that the best cancer hospital in Delhi is the right place to find the best oncologist in Delhi. Equipped with the highest qualifications and ably assisted by an efficient support staff, the oncologists at the world-class Indraprastha Apollo Hospital provide cancer patients the best care possible. The top-end facilities, equipment and techniques available to a cancer specialist here go a long way in strongly backing the healing process of every patient.
Besides qualifications and experience, empathy and compassion are equally important qualities to look for in the best oncologist in Delhi. At the Indraprastha Apollo Hospital, each member of the Apollo Cancer Institute is committed to providing cancer patients with every life-saving treatment available. For example, Image Guided Radiotherapy (IGRT), Stereotactic Body Radiotherapy (SBRT), Frameless Stereotactic Radiosurgery (SRS), 3D Conformal Radiotherapy, Intensity Modulated Radiotherapy (IMRT), and High Dose Rate (HDR) Brachytherapy are offered here for early detection of cancer and advanced surgical technology known as da Vinci robotical surgical system help cancer surgeons perform complicated surgeries with ease ensuring best outcome. In addition, the Tumour Board and Group Tumour Board meetings foster discussions between surgical, medical and radiation oncologists as do the Cancer Awareness Programs and counselling sessions offered at the Apollo Cancer Institute.
Follow-up constitutes an important component of treatment and is an integral part of the management protocols carried out by the Apollo Cancer Institute. Early detection and timely management of recurrence is the principle objective of follow-up in cancer management. The best oncologist in Delhi firmly believes this not only enhances survival but improves quality of life of patients.
Take a look at some of the top cancer specialists at Indraprastha Apollo Institute, who would each qualify to be the best oncologist in Delhi:
Dr Anil D’Cruz
MBBS, MS, DNB, FRCS (HON.
With over three decades of experience, Dr D’Cruz is a renowned surgical oncologist focusing primarily on head and neck cancers. His major areas are management of neck metastasis, conservative laryngeal surgery, cancers of the oral cavity, thyroid, quality of life issues and global health.
Dr Manish Singhal
MBBS, MD, DM(AIIMS)ECMO
Dr Singhal’s career spans over twenty years, largely covering all types of chemotherapy, intensive protocols, immunotherapy, hormonal therapy in addition to dealing with oncological emergencies, including medical care of patients.
Dr Dipanjan Panda
MBBS, MD, DM
One of the best medical oncologists in Delhi, Dr Panda’s area of expertise lies in gastrointestinal and hepatic pancreatico biliary malignancy, breast and gynaecological malignancy, lung and head neck cancer, genito-urinary malignancy, lymphoma and myeloma (haematological malignancy) and rare tumours like neuroendocrine tumours.
Dr Shuaib Zaidi
MBBS, MS (SURGERY), DNB (SURGERY), MCH (SURGICAL ONCOLOGY)
The Academic Coordinator and Senior Consultant in the Department of Surgical Oncology, Dr Zaidi has over twenty years of experience as a surgical oncologist. He specialises in the treatment of thoractic cancer, gastrointestinal cancer, PIPAC (Pressurised Intraperitoneal Chemotherapy), breast cancer and complex gynaecologic oncology.
Dr Praveen Garg
MBBS, M.S.(GEN.SURGERY), M.CH.(ONCOSURGERY)
Dr Garg specialises in the diagnosis, treatment and surgical management of malignant conditions in various parts of the body, and has advanced training in parathyroid and thyroid cancer surgeries, breast conservation surgeries, mastectomies and breast tissue reconstructions.
Dr Ruqaya Ahmed Mir
MBBS, DNB
Trained in robotic surgery, Dr Mir routinely performs major oncological resectional surgical procedures for head and neck cancers, lung and oesophageal cancers, major gastrointestinal malignancies, breast and gynaecological malignancies and soft tissue sarcomas.
To get in touch with the best oncologist in Delhi, contact Indraprastha Apollo Hospital
2 notes
·
View notes
Text
Recurrent or Persistent Hyperparathyroidism
Recent cure rates of hyperparathyroidism following parathyroidectomy: Are reported between 92% and 97% When cure is not obtained, it is due to either: Recurrent or persistent disease (Figure) Persistent hyperparathyroidism: Is defined as hypercalcemia and elevated parathyroid hormone (PTH) levels: During the 6-month period after parathyroidectomy: It occurs in 0.4% to 7.8% of…

View On WordPress
0 notes
Text
Story at-a-glance
Over 50% of Americans are magnesium deficient, and nearly half the global population lacks adequate calcium intake, raising the risk of cognitive issues ranging from memory lapses to severe impairments
Magnesium powers brain cell energy production, acts as an antioxidant and regulates NMDA receptors for memory formation, with research showing higher levels correlate with better cognitive performance
Calcium plays a key role in neurotransmission and memory formation, with low levels linked to increased risks of cognitive decline and neurodegenerative diseases
Low dietary calcium triggers parathyroid hormone release, causing calcium to be pulled from bones and deposited in soft tissues — contrary to common beliefs about calcium supplementation causing calcification
Vitamins D3 and K2 work synergistically with calcium and magnesium to ensure proper absorption and direct calcium to bones rather than soft tissues and arteries; a balanced calcium-to-phosphorus ratio is also important
0 notes